How to Write a Public Health Dissertation: The Complete MPH Guide (2026)
Writing a public health dissertation is one of the most demanding — and most rewarding — academic projects you will undertake in your MPH or undergraduate public health programme. Unlike dissertations in the humanities, a public health project must marry rigorous research methodology with real-world relevance: your findings should, in principle, be usable by a health department, a policy-maker, or a community organisation. That combination of scientific rigour and societal impact is what makes the MPH dissertation uniquely challenging and uniquely satisfying.
This guide walks you through every stage of the process, from choosing a topic that is both personally motivating and academically feasible, to selecting the right research design, navigating ethics approval, finding the best open-access data sources, and structuring every chapter so your examiner can see the quality of your thinking. Whether you are at Harvard T.H. Chan, the London School of Hygiene & Tropical Medicine, the University of Edinburgh, or any other programme worldwide, the core principles here apply to your dissertation.
1. What Is a Public Health Dissertation?
Video: How to write your dissertation — MPH Manchester
A public health dissertation is an original, independent research project submitted as the culminating requirement of a Master of Public Health (MPH), an MSc in Public Health, or a senior undergraduate public health degree. At the University of Edinburgh, for example, the MPH dissertation is described as “an extended piece of scholarship demonstrating research skills and critical engagement with public health literature.” Most programmes expect a word count between 10,000 and 15,000 words for master’s projects, though some research-intensive programmes allow up to 20,000 words.
What distinguishes a public health dissertation from a generic social-science thesis is its commitment to health relevance. Every methodological decision — your research question, your population, your outcome measure — should connect explicitly to a public health need, an equity concern, or a policy gap. Examiners at LSHTM, Harvard, and similar institutions are not just assessing your ability to conduct research; they are assessing whether your research could plausibly inform action.
Dissertation vs. Research Portfolio
Some MPH programmes, particularly in the United States, offer a non-thesis “Applied Practice Experience” route. This guide focuses on the dissertation or thesis track, which involves original research and independent analysis rather than a practice placement report.
2. Choosing Your Dissertation Topic
Topic selection is the single most consequential decision you will make. A poorly chosen topic — too broad, too data-sparse, or misaligned with available supervision — can derail even the most talented student. Here is a structured approach used by many successful MPH candidates.
Step 1: Start with a Public Health Problem, Not a Method
Begin by identifying a health problem that you find genuinely important. According to guidance from programmes including the University of Washington’s Department of Global Health, the best dissertation topics are driven by personal passion — writing a master’s dissertation takes many months, and sustained motivation requires genuine investment in the question. Ask yourself: Which disease burden, health inequality, or policy failure keeps you engaged when you read the news?
Strong starting points include:
- Disease-specific research (e.g., antimicrobial resistance, childhood obesity, mental health in refugees)
- Health systems and policy (e.g., access to primary care, vaccination hesitancy, health financing)
- Social determinants and equity (e.g., housing and respiratory disease, income inequality and diabetes prevalence)
- Global health and international comparisons (e.g., maternal mortality across low- and middle-income countries)
- Environmental and occupational health (e.g., air pollution and cardiovascular outcomes, heat stress in outdoor workers)
Step 2: Check Feasibility Against Four Constraints
Once you have a broad area, test every candidate topic against these four constraints before committing:
| Constraint | Key Question |
|---|---|
| Data availability | Does a usable dataset exist (WHO, CDC, NHS Digital, national health surveys), or can you collect data within your timeline? |
| Supervision expertise | Is there a supervisor at your institution who has methodological experience with your chosen design? |
| Ethics timeline | Will your study require full ethics review, and can it be approved before your data-collection window opens? |
| Scope | Can the question be answered meaningfully within your word limit and time allocation? |
Step 3: Formulate a PICO or PECO Research Question
Structured frameworks help you move from a broad topic to a specific, answerable research question. Two frameworks dominate in public health:
- PICO (Population, Intervention, Comparator, Outcome) — used for intervention studies and systematic reviews of effectiveness
- PECO (Population, Exposure, Comparator, Outcome) — used for observational and epidemiological studies examining risk factors or associations
Example PECO question: Among adults aged 40–65 in urban England (Population), is long-term exposure to PM2.5 air pollution (Exposure) compared to low exposure (Comparator) associated with higher incidence of type 2 diabetes (Outcome)?
3. Common Research Designs for Public Health Dissertations
Public health research uses a wider range of designs than almost any other discipline. The University of Edinburgh’s MPH programme, for instance, explicitly supports quantitative data analysis, systematic literature review, and qualitative research as the three main dissertation tracks. Understanding the strengths and limitations of each will help you select the most appropriate fit for your question.
Systematic Review (with or without Meta-Analysis)
A systematic review comprehensively identifies, appraises, and synthesises all available evidence on a focused question. It is one of the most respected designs in public health because it sits at the top of the evidence hierarchy and can directly inform clinical guidelines or policy. For an MPH dissertation, a systematic review is feasible without primary data collection, which removes many logistical barriers — though the literature-searching and quality-appraisal stages are demanding in their own right.
When to choose this design: When you want to answer “Does X intervention work?” or “Is Y risk factor associated with Z outcome?” and sufficient primary studies already exist to be synthesised.
Key tool: The PRISMA 2020 reporting guideline — discussed in Section 6 below.
Secondary Data Analysis
Secondary data analysis involves analysing an existing dataset that was collected for a purpose other than — or broader than — your specific research question. This is the most common quantitative design for MPH dissertations at Edinburgh, Harvard, and many other programmes, because it provides access to large, representative, high-quality datasets without the time and cost of primary data collection.
Typical datasets: National Health and Nutrition Examination Survey (NHANES), Health Survey for England, WHO Global Health Observatory, Demographic and Health Surveys (DHS), BRFSS (Behavioral Risk Factor Surveillance System).
When to choose this design: When a high-quality existing dataset contains the exposure and outcome variables that match your PECO question and your programme has — or can facilitate — access to it.
Epidemiological Study (Primary Data Collection)
Primary epidemiological studies — cross-sectional surveys, case-control studies, cohort studies — involve collecting original data from participants. They offer the most direct control over variables and measurement quality, but they require more time, more substantial ethics review, and realistic participant access. For most MPH programmes, a cross-sectional survey is the most achievable primary-data design within a one-year programme.
When to choose this design: When no existing dataset adequately captures your exposure or population, and you have access to a sufficient sample — for example, through a health authority partner or a community organisation.
Qualitative Research
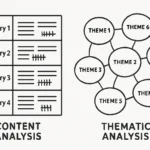
Qualitative designs — including semi-structured interviews, focus groups, thematic analysis, and ethnographic observation — are used when the research question is exploratory and concerned with understanding experiences, perceptions, or processes rather than measuring frequency or association. They are particularly valuable for health behaviour research, implementation science, and studies of marginalised communities whose experiences are not captured by large survey datasets.
Common methods: Framework analysis, thematic analysis (Braun and Clarke), interpretative phenomenological analysis (IPA), grounded theory.
When to choose this design: When you want to answer “How?”, “Why?”, or “What does it mean?” rather than “How many?” or “How much?”
Mixed Methods
Some MPH dissertations combine a quantitative strand (e.g., a survey measuring prevalence) with a qualitative strand (e.g., interviews exploring barriers to care) in a sequential or concurrent design. Mixed methods are ambitious for a one-year programme but can be achieved if the quantitative component is secondary data analysis — reducing the data-collection burden — and the qualitative component involves a small, purposive sample. For a deeper treatment of design justification across any of these tracks, see our guide on how to write a research methodology chapter.
4. Ethics Approval and IRB/REC Considerations
Ethics review is not a bureaucratic hurdle — it is a fundamental commitment to participant welfare, scientific integrity, and public trust. In the United Kingdom, research involving NHS patients or their data requires Health Research Authority (HRA) approval and Research Ethics Committee (REC) review. In the United States, institutional research involving human subjects requires Institutional Review Board (IRB) approval under federal regulations (45 CFR 46). Many other countries have equivalent national or institutional processes.
What Level of Review Does Your Study Need?
| Study Type | Typical Ethics Level (UK/US) | Timeline |
|---|---|---|
| Systematic review of published literature | Usually exempt / no REC needed | Days (institutional sign-off only) |
| Secondary analysis of anonymised open-access data (NHANES, WHO GHO) | Exempt (US) / no HRA needed (UK) | Weeks |
| Online survey, healthy adult volunteers, no sensitive topics | Institutional REC (light review) | 4–8 weeks |
| Interviews on sensitive topics, vulnerable populations, NHS access | Full REC / HRA (UK) or Full IRB (US) | 2–4 months |
The key lesson: match your ambition for primary data collection to your actual ethics timeline. If your programme’s data-collection window opens in April and full REC review takes three months, you must submit your ethics application no later than January — ideally before Christmas.
Informed Consent
All primary research involving human participants requires written or documented informed consent. Your consent form and participant information sheet must clearly state: the study purpose, what participation involves, data storage and confidentiality arrangements, the right to withdraw at any time without consequence, and your contact details and those of your supervisor. Most UK universities provide templates; adapt them to your specific study, do not simply copy them verbatim.
Data Protection
In the United Kingdom, any research involving personal data must comply with the UK General Data Protection Regulation (UK GDPR) and the Data Protection Act 2018. In the European Union, GDPR applies. In the United States, HIPAA governs protected health information. Anonymising or pseudonymising data at the earliest opportunity, storing it on encrypted, institution-managed drives, and specifying a clear data-retention period are standard good-practice steps that almost all ethics committees will expect to see.
5. Key Data Sources: WHO, CDC, and National Health Surveys
One of the most significant advantages of a public health dissertation — compared to, say, a psychology or sociology project — is the abundance of free, high-quality, publicly available datasets curated by international health organisations and national governments. Knowing where to look can transform a project that seems data-impossible into one that is achievable within weeks.
WHO Global Health Observatory (GHO)
The WHO Global Health Observatory is the World Health Organization’s primary health statistics repository, providing data on more than 1,000 indicators across WHO’s 194 member states. The GHO covers mortality and burden of disease, nutrition, reproductive health, substance use, health service coverage, and more. Data can be filtered by country, region, year, and indicator, and downloaded in CSV or Excel format. The GHO also supports an OData API for more complex queries. For dissertations on global health comparisons, SDG monitoring, or cross-national epidemiology, the GHO is often the single best starting point.
CDC Data and Statistics
The US Centers for Disease Control and Prevention maintains several major public datasets:
- NHANES (National Health and Nutrition Examination Survey) — combines interview and physical examination data for a nationally representative US sample; covers diet, physical activity, laboratory results, and chronic disease diagnoses
- BRFSS (Behavioral Risk Factor Surveillance System) — the largest continuously conducted health survey in the world, covering health-risk behaviours, chronic conditions, and use of preventive services
- WONDER (Wide-ranging ONline Data for Epidemiologic Research) — mortality, natality, cancer, and environmental data for the United States
UK and International Sources
- NHS Digital / NHS England — hospital episode statistics, GP prescribing data, cancer registry data
- Health Survey for England — annual survey of health and health-related behaviours in adults and children
- CPRD (Clinical Practice Research Datalink) — anonymised UK primary care records; access requires an application but is free for academic projects
- IHME Global Burden of Disease (GBD) — comparative estimates of mortality, morbidity, and risk factors across 200+ countries
- Demographic and Health Surveys (DHS) Programme — nationally representative surveys in low- and middle-income countries on population, health, and nutrition
- Eurostat — European Union health statistics and health determinants data
6. Reporting Guidelines: PRISMA 2020 and STROBE
Reporting guidelines are evidence-based checklists that specify the minimum information a study must report so that readers can assess its validity and replicate its methods. Using the correct guideline for your study design is not optional — most examiners, and virtually all journals, expect to see compliance. The EQUATOR Network (equator-network.org) is the definitive online library of over 500 reporting guidelines; it should be your first stop.
PRISMA 2020 (Systematic Reviews and Meta-Analyses)
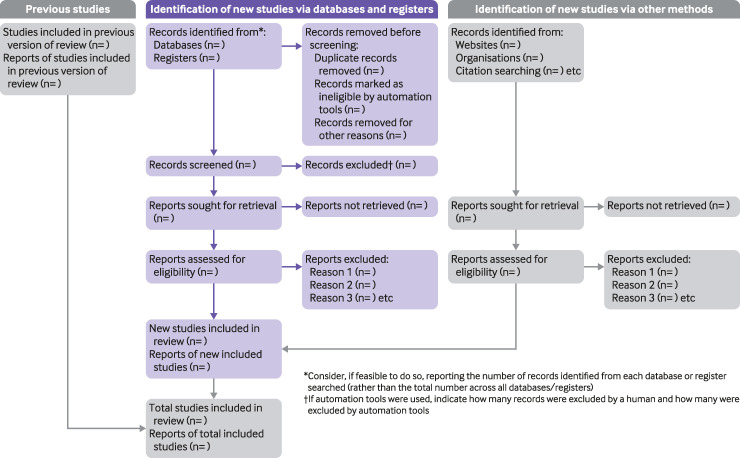
The Preferred Reporting Items for Systematic Reviews and Meta-Analyses statement was substantially updated in 2020 to reflect advances in systematic review methodology. The PRISMA 2020 statement includes a 27-item checklist, an abstract checklist, and revised flow diagrams for original and updated reviews. Key items that MPH students often miss include:
- A completed PRISMA flow diagram showing the number of records identified, screened, assessed for eligibility, and included
- Pre-registration of the review protocol on PROSPERO (International Prospective Register of Systematic Reviews)
- A risk-of-bias assessment for each included study, using a validated tool such as the Cochrane RoB 2 tool or the Newcastle-Ottawa Scale
- Assessment of publication bias, where applicable (e.g., funnel plot, Egger’s test for meta-analyses)
The PRISMA 2020 checklist has been cited in over 60,000 reports and endorsed by almost 200 journals — it is the global standard for systematic review reporting.
STROBE (Observational Studies in Epidemiology)
The Strengthening the Reporting of Observational Studies in Epidemiology statement provides a 22-item checklist covering cohort studies, case-control studies, and cross-sectional studies. It is the standard guideline for primary epidemiological research and secondary data analyses using observational study designs. Items specific to observational studies that students frequently under-report include:
- Explicit description of the study design in the title or abstract
- Eligibility criteria and sources and methods of selection of participants
- How exposures and outcomes were measured, including any validation
- Statistical methods, including methods to address confounding
- Efforts to address potential sources of bias
A study evaluating STROBE compliance in published observational research has shown that reporting quality improves substantially when researchers use the checklist proactively during drafting, rather than as a post-hoc review. Apply it chapter by chapter, not only at the end.
Other Guidelines Worth Knowing
| Guideline | Study Type |
|---|---|
| CONSORT 2010 | Randomised controlled trials |
| COREQ | Qualitative research (interviews, focus groups) |
| SRQR | Qualitative research (broader scope) |
| TREND | Non-randomised evaluations of behavioural and public health interventions |
7. Chapter-by-Chapter Dissertation Structure
Most public health dissertations follow a broadly similar structure, though specific chapter titles and requirements vary by programme and design. The template below reflects the expectations of leading MPH programmes including those at Harvard T.H. Chan, LSHTM, and the University of Edinburgh. Adapt it to your programme’s submission guidelines.
Title Page and Abstract
The abstract is the most-read part of your dissertation. It should be structured (Background, Methods, Results, Conclusions) and no longer than 300 words. State your focus keyword — the precise research question — in the first sentence, and end with a single sentence on the policy or practice implication of your findings. Do not include citations in the abstract.
Chapter 1: Introduction
The introduction does four things: (1) establishes the public health significance of your topic with relevant context and burden-of-disease figures; (2) identifies the gap in knowledge that your study addresses; (3) states your aims and objectives clearly; and (4) provides a brief overview of the dissertation structure. The introduction is typically 1,000–1,500 words. Avoid summarising your results here — that belongs in the abstract and the discussion.
Chapter 2: Literature Review
The literature review critically evaluates what is already known about your topic. This is not a descriptive summary of papers — it is an analytical synthesis that identifies consistent findings, contradictions, methodological limitations, and gaps that justify your study. Use a systematic or structured search strategy (database names, search terms, date limits, inclusion criteria) so your reviewer can understand how you identified your sources. In a systematic review dissertation, this chapter becomes the central analytical body of the work and must follow PRISMA 2020 in full.
Chapter 3: Methodology
The methodology chapter is where examiners assess your research literacy most rigorously. Cover:
- Study design — name it explicitly (e.g., “retrospective cross-sectional secondary data analysis”) and justify why it is appropriate for your question
- Data source — describe the dataset in detail (who collected it, how, in what years, how participants were sampled)
- Study population — eligibility criteria (inclusion and exclusion), sample size, and any missing-data strategy
- Variables — how each exposure, outcome, and covariate is defined and measured in the dataset
- Statistical or analytical approach — specify the software (R, Stata, SPSS, Python) and the analytical procedures (e.g., logistic regression, Poisson regression, thematic analysis)
- Ethical considerations — state the ethics approval reference number or the basis for exemption
The methodology chapter should be detailed enough that another researcher could replicate your study. If you are conducting a systematic review, register your protocol with PROSPERO before beginning your search. For a thorough guide on framing your study’s constraints honestly, see our article on how to write a research limitations section.
Chapter 4: Results
Present your findings in a logical order — usually from descriptive statistics (characteristics of your study population) through to inferential analyses (associations, themes, or synthesised evidence). Use tables and figures to communicate complex data efficiently, but never leave them to speak for themselves: every table and figure needs an accompanying text explanation of the key finding. Report according to your relevant guideline (PRISMA flow diagram for systematic reviews, STROBE-aligned results for observational studies). Do not interpret your results here — save that for the discussion.
Chapter 5: Discussion
The discussion is the intellectual core of your dissertation. Structure it around four moves:
- Summary of principal findings — a brief, non-technical restatement of what you found
- Comparison with existing literature — do your findings align with, contradict, or extend prior evidence? Explain why discrepancies might exist
- Strengths and limitations — be honest and specific; every study has both, and examiners credit intellectual honesty over defensive evasion
- Public health implications — what should practitioners, commissioners, or policy-makers do differently in light of your findings?
Chapter 6: Conclusion
The conclusion draws together the threads of the dissertation in 500–800 words. It should restate your research question, briefly summarise what you found and its significance, and indicate directions for future research. Avoid introducing new evidence or arguments in the conclusion. For practical guidance on writing future research directions that impress examiners, see our guide on how to write recommendations for future research — it covers the five-step derivation process and discipline-specific worked examples.
References and Appendices
Most public health programmes accept Vancouver or APA referencing, though some (particularly those aligned with epidemiology journals) use Vancouver exclusively. Check your programme handbook. Appendices should include your ethics approval letter or exemption confirmation, your data access agreement, any survey instruments you created, and supplementary tables that would break the flow of the results chapter if placed in the main body.
8. Writing and Time-Management Tips
The University of Edinburgh’s MPH programme allocates 6–10 hours of supervisor contact across the dissertation period — a reminder that the dissertation is fundamentally an independent project. Most students are surprised by how much of the work is writing, not just analysis. Here are strategies that work at every stage.
Build a Realistic Timeline
Work backwards from your submission deadline. A rough guide for a one-year MPH:
- Months 1–2: Topic selection, proposal writing, supervisor agreement, ethics submission
- Months 3–4: Literature search and review, finalise methodology
- Months 5–6: Data access, data cleaning, analysis
- Months 7–8: Draft results and discussion chapters
- Month 9: Complete introduction and conclusion; full draft to supervisor
- Month 10: Revisions based on supervisor feedback; proofreading; formatting
- Month 11: Final submission
Write Every Day, Even Briefly
Daily writing beats weekend marathons. Even 30 minutes of focused writing per day produces 200–400 words — which adds up to 6,000–12,000 words over a month. Use a writing log to track your daily progress and build a habit that prevents the blank-page paralysis that strikes many students in the final two months.
Use Your Methodology Chapter as Your Anchor
Many experienced supervisors advise writing the methodology chapter first, before your analysis is complete. Articulating your methods in writing often reveals gaps or ambiguities in your analytical plan that are much easier to fix before you have begun analysis than after. It also gives you a sense of progress and a concrete reference point for all subsequent chapters.
Work With Your Supervisor’s Feedback Systematically
When your supervisor returns a draft with comments, resist the temptation to implement changes immediately and ad hoc. Instead, read all comments first, categorise them (structural issues vs. clarity edits vs. content additions), and address them in a single planned revision pass. This approach reduces the risk of introducing new inconsistencies while fixing old ones.
Use Reference Management Software from Day One
Zotero (free, open-source) and Mendeley are both widely used by public health students. Set up your reference library before you begin your literature search, not after — retroactively adding citations to a 200-reference library is painful and error-prone. For systematic reviews, Rayyan or Covidence (free for students at many institutions) streamlines the title-and-abstract screening process considerably.
Frequently Asked Questions
How long should a public health dissertation be?
Most MPH dissertations are between 10,000 and 15,000 words, excluding references and appendices. The University of Edinburgh, for example, specifies 12,000 words for their MPH dissertation. Some research-intensive programmes allow up to 20,000 words. Always check your specific programme handbook, as word limits vary significantly and exceeding them without permission can affect your mark.
Can I do a systematic review as my MPH dissertation?
Yes — a systematic review is one of the most common and highly valued MPH dissertation designs. It does not require primary data collection, which makes it logistically straightforward. However, it demands a rigorous and transparent search strategy, a pre-registered protocol (ideally on PROSPERO), quality appraisal of included studies, and a structured synthesis reported according to PRISMA 2020. Confirm with your supervisor that sufficient primary studies exist on your question before committing to this design.
Do I need ethics approval for secondary data analysis?
In most cases, secondary analysis of anonymised, publicly available datasets (such as NHANES, WHO GHO, or the Health Survey for England) is exempt from full ethics review in both the UK and the US. However, you will still need to obtain written confirmation of exemption from your institution’s ethics committee and comply with the data use terms of the dataset (which typically prohibit re-identification). Always confirm the ethics route with your supervisor and your institution’s research ethics office before downloading data.
What is the difference between PRISMA and STROBE?
PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) is the reporting guideline for systematic reviews and meta-analyses — studies that synthesise results across multiple primary studies. STROBE (Strengthening the Reporting of Observational Studies in Epidemiology) is the reporting guideline for individual observational studies: cohort studies, case-control studies, and cross-sectional studies. If your dissertation involves reviewing and synthesising existing literature, use PRISMA 2020. If you are conducting an original epidemiological study — primary or secondary data — use STROBE. Both checklists are available free at the EQUATOR Network website.
How do I choose between a quantitative and qualitative approach for my public health dissertation?
The choice should follow your research question, not your methodological comfort zone. If you want to measure prevalence, test associations between exposures and outcomes, or synthesise effect estimates across studies, a quantitative approach is appropriate. If you want to understand experiences, explore how people make health decisions, or investigate why a policy was or was not implemented, a qualitative approach is more suitable. A mixed-methods design can address both types of question but requires more time and supervisory expertise. When in doubt, discuss the options with your supervisor before finalising your proposal.
Which statistical software should I use for my public health dissertation?
R (free, open-source) and Stata are the most widely used in academic public health research and are preferred by most MPH programmes, including those at Harvard T.H. Chan, LSHTM, and the University of Edinburgh. R is particularly powerful for data visualisation and reproducible analysis, while Stata’s survey analysis commands are excellent for complex sample designs like NHANES. SPSS is still accepted at many institutions but is less commonly used in research-intensive programmes. Python is increasingly popular for large-dataset analyses. Whichever software you choose, ensure you can justify your choice in your methodology chapter and that your supervisor has expertise in it.
Ready to Start Your Public Health Dissertation?
Writing a public health dissertation requires careful planning, methodological rigour, and a lot of sustained effort — but you do not have to do it alone. Tesify is an AI-powered academic writing tool built specifically for thesis and dissertation students. Whether you are drafting your literature review, structuring your methodology chapter, or polishing your discussion, Tesify helps you write with more clarity, confidence, and speed.
Write your thesis with AI
Structure, draft, cite, and format your thesis faster with Tesify’s AI writing tools, automatic bibliography, and plagiarism checker. Free to start, no credit card required.

Leave a Reply